The most common instability of the shoulder joint is acute acquired instability. This means that an accident causes the shoulder to either subluxate or luxate entirely. The accident damages the capsule and ligaments that limit movements in the shoulder joint. The most common direction of dislocation is forward resulting in anterior shoulder instability. Besides acute instability, 2 other mechanisms can cause shoulder instability.
In this article, I’ll discuss why the shoulder usually dislocates forward, the 3 types of mechanisms underlying it, and how to deal with shoulder instability as a rock climber.
Let’s dive right in.
1. Anatomy of the Shoulder Joint
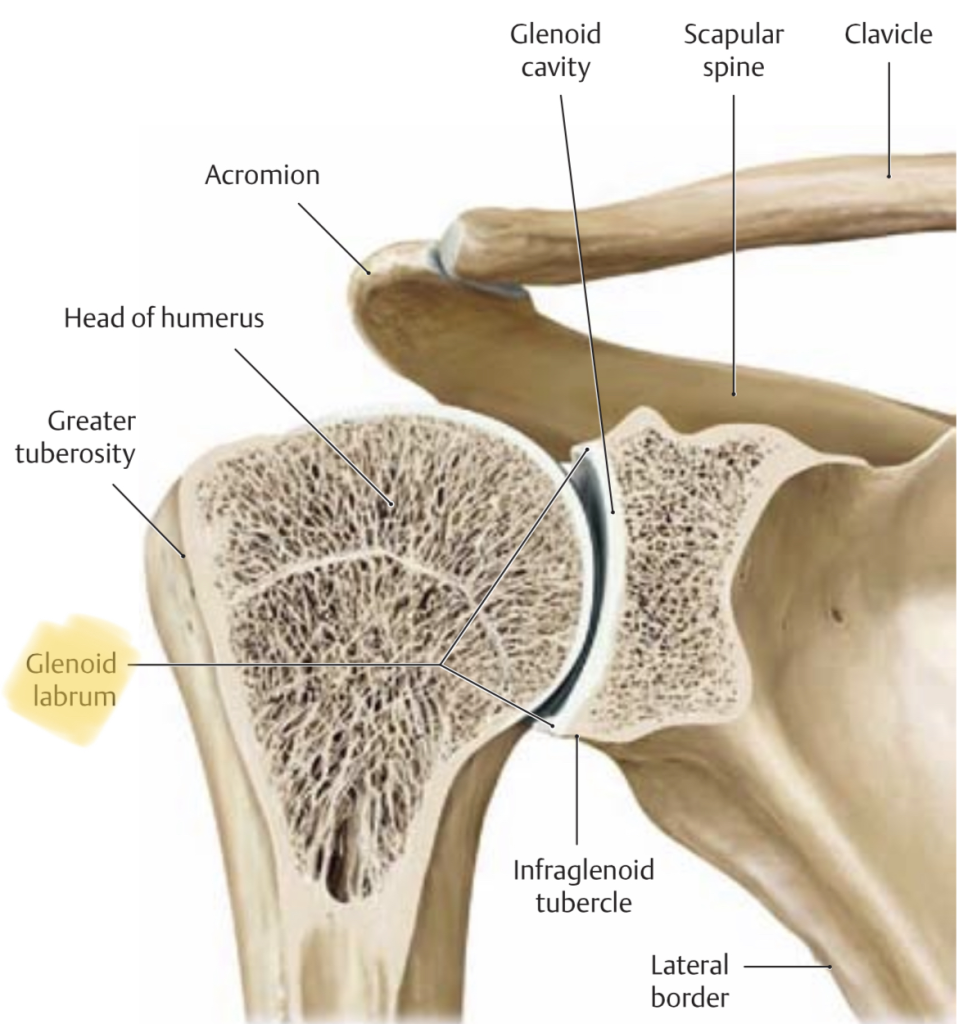
The shoulder joint, or the glenohumeral joint, is a ball and socket joint. The socket, or glenoid, is on the lateral side of your scapula and the ball is the head of the humerus, your upper arm. The socket on the scapula is flat and layered with cartilage. A spongy type of bone that helps to protect the underlying bone and works as a shock absorber. Around the edge of the glenoid, there’s an extra edge of cartilage called the labrum. This layer adds stability to the shoulder joint.
Since the glenoid is flat you can move the shoulder as freely as you can. The downside is that it’s prone to stability issues if it doesn’t function as it should. For example, this is different in the hip, where the acetabulum is a deep socket for the femur providing plenty of stability.
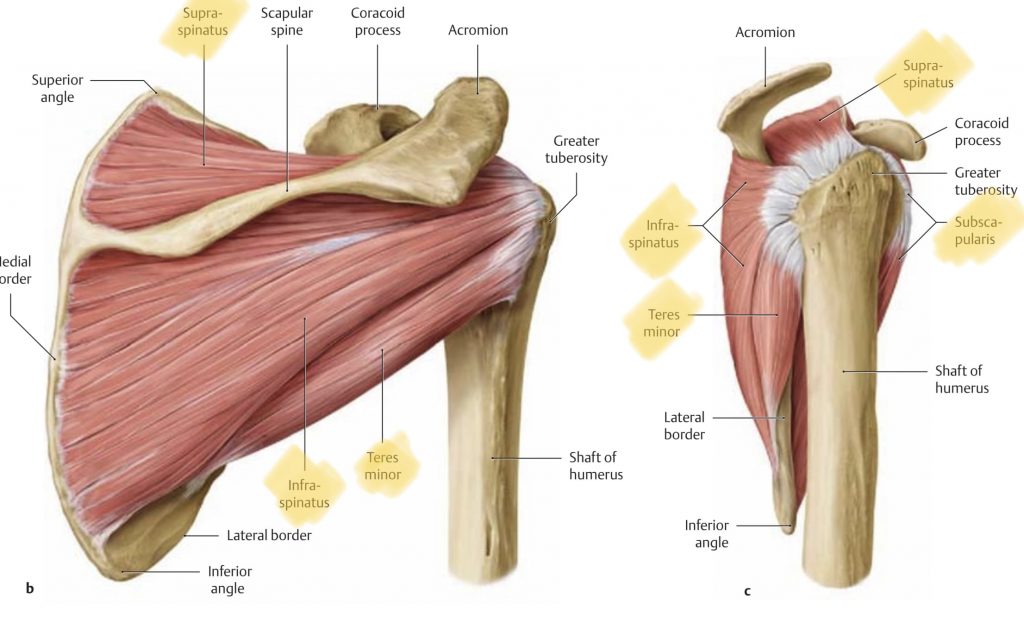
Besides the labrum, the Superior, Medial, and Inferior Glenohumeral Ligaments add to the passive stability of the shoulder joint. The active stability comes from the rotator cuff muscles, the supraspinatus, infraspinatus, teres minor, and subscapularis. These 4 muscles work together tightly to centralize the humerus on the glenoid during movement. The better these muscles do their job the less likely you experience instability.
Before we move on to the shoulder instability mechanisms, what exactly is shoulder instability?
2. What is Shoulder Instability?
Shoulder instability is defined as when shoulder joint laxity causes symptoms:
- An unstable sensation in certain positions
- A sense of weakness in the shoulder joint either in general or in certain positions
- Fear of moving into certain positions
- (Sub)luxation of the humerus with or without an actual trauma
3. Instability Mechanisms
According to the literature, there are 3 shoulder instability mechanisms:
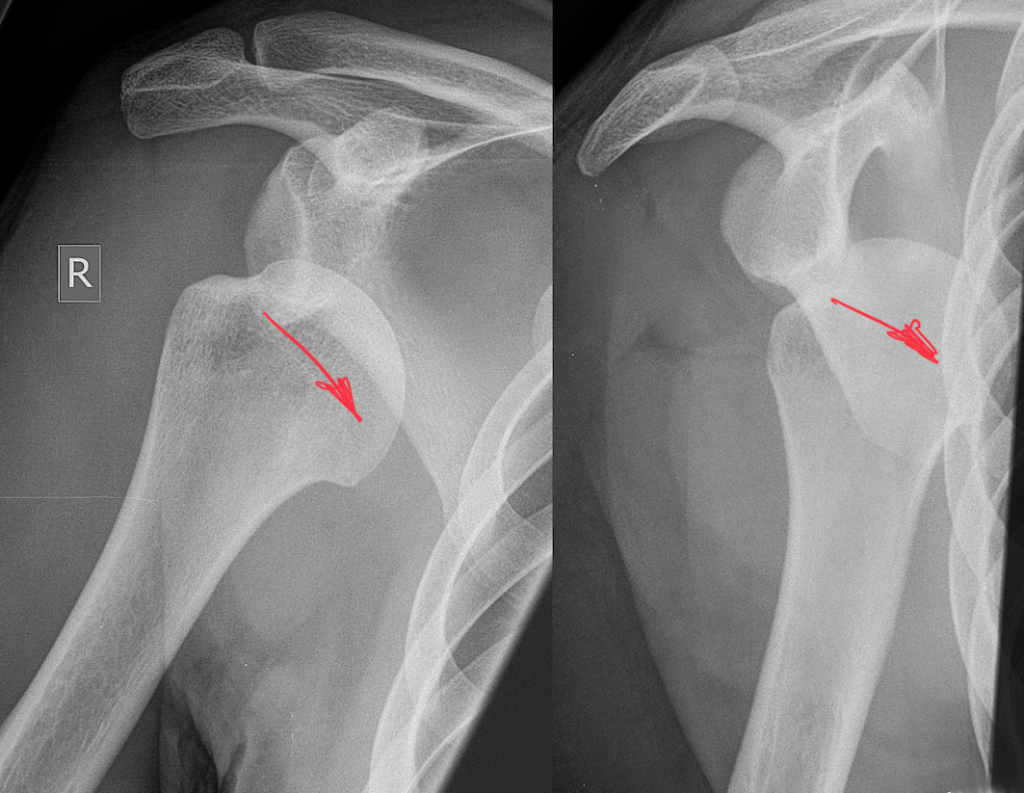
- Traumatic shoulder instability is due to an accident during which you (sub)luxated your shoulder, damaging the humerus, labrum, ligaments, muscles, and/or tendons. For example, the Hill-Sachs lesion (damage to the humeral head) and the Bankart Lesion (damage to the labrum).
- A-traumatic shoulder instability is also called Multidirectional Instability (MDI) and can either be congenital or acquired, meaning that one or both shoulders have lax(er) passive structures. This can be congenital or otherwise, in overhead athletes like rock climbers and swimmers’ shoulder joint laxity is the result of repeated overhead movements.
- Functional Shoulder Instability (FSI) is a disturbance in the coordination of the muscles that stabilize the shoulder joint.
4. Risk Factors for Acquiring Shoulder Instability
There are several risk factors for shoulder instability:
- Contact/Overhead sports
- Rotator Cuff weakness
- Congenital shoulder joint or generalized joint laxity
- Monotonous training (as a rock climber this means you do nothing else than rock climbing and/or bouldering)
- Previous shoulder (sub)luxations
- Younger age (children/youth have more elastic tissues than people over 30-35)
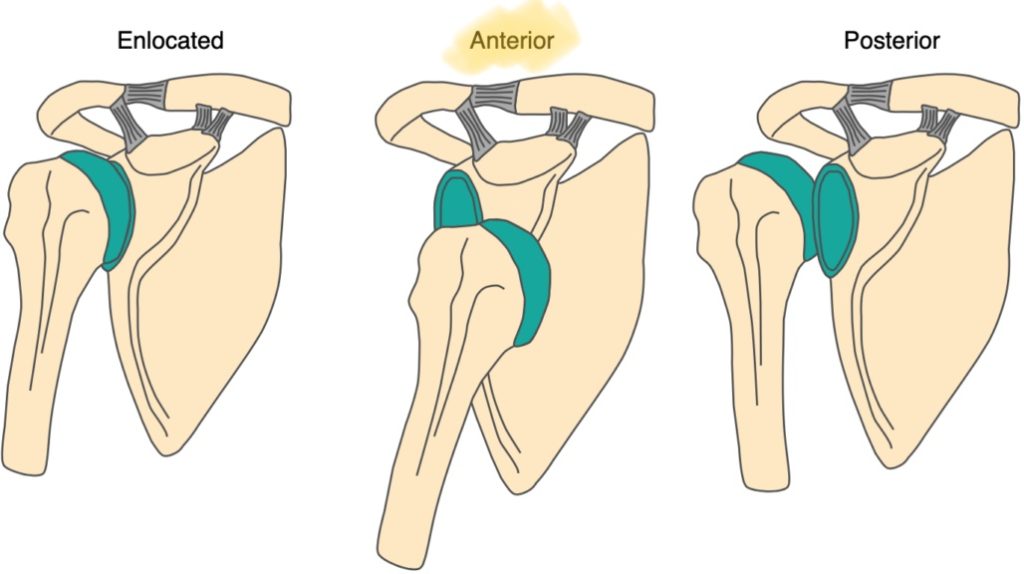
5. Why is Anterior Shoulder Instability Most Common?
To understand why anterior shoulder instability is the most common you have to understand how the shoulder joint works; when you externally rotate your shoulder the head of the humerus slides forward. This is limited though by the structures at the front of the shoulder so that the humerus always stays as centrally as possible on the glenoid. This ensures optimal stability and mobility. The problem is though that most of our activities are with the arm abducted and externally rotated while the shoulder joint, as I’ve mentioned above, has no inherent stability. The result is that your shoulder sub-luxates/dislocates almost always luxates in the direction where it moves most.
This is confirmed by a scientific paper on unstable shoulders in adolescent athletes. Anterior dislocations and subluxations of the shoulder joint account for 98% of the cases whereas posterior dislocations only happen in 2% of the accidents.
In rock climbers, sudden wrenching movements are the most common reason for acute shoulder instability. Examples of these are:
- Slipping off a foothold which causes a sudden pull on your shoulder
- Placing your hand in the external rotation behind your body and putting a lot of pressure on the arm
- Placing your hand in external rotation while having the arm abducted 90 degrees or more and putting a lot of pressure on the arm
6. Shoulder Instability in Rock Climbers
Even if you never experienced an accident with your shoulder, it’s still likely that you as a rock climber have at least to some degree generalized laxity of the shoulder joint due to repetitive overhead movement.
Most rock climbers still get their arms overhead well even though they have the “climber’s back”. This is the exaggerated kyphosis (rounding) of the thoracic spine and the protracted shoulder girdle because of frequent pulling. This prominent kyphosis prevents the necessary extension in the thoracic spine to elevate your arm overhead. When your shoulder joints are more flexible, you can compensate for the lack of mobility in your back.
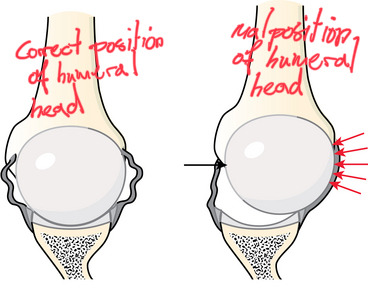
The downside of shoulder laxity is that the head of the humerus is more likely to be positioned forward in the shoulder joint. This makes the joint less stable and is thus more prone to acute injuries.