Climbing injuries in the wrist can be painful, provoke a sense of instability, and reduce wrist and hand mobility. It depends on the injured structure which is the best course of treatment. In all cases, figure out why your wrist hurts so you can choose the right treatment. Climbing through pain is never smart and can force you to stop your actual climbing at best or cause long-term damage in the worst case.
So, in this blog, I discuss the knowledge and tools to help you in the right direction to heal your injury. Still, this is not a substitute for real medical care, so use this information to choose the right approach with the right medical professional.
With that being said, let’s dive in right away!
1. Wrist Injuries from Rock Climbing
Like with all injuries, you can divide wrist injuries from rock climbing into 2 groups:
- Acute
- Chronic
Acute injuries are usually accidents, or there’s an acute onset of your pain otherwise. Chronic injuries come on slowly and might become evermore prominent and evermore limiting. These are often a result of overload over a longer period.
The acute wrist injuries I’ll discuss in this blog are:
- Distal Radius Fracture
- Fracture of Hamatum
The injuries with a slow onset are:
- Bone Marrow Edema
- Carpal Tunnel Syndrome
- Morbus Dupuytren
- Tenosynovitis
- Ulnocarpal Pain Syndrome
And remember, that injuries with a slow onset might present themselves suddenly. Which might lead you to believe it’s an acute injury. In reality, it has been cooking under the surface for a while already.
2. Distal Radius Fracture
The distal radius fracture is the most obvious of all the injuries I discuss in this blog. You fall with outstretched arms to the floor, most likely when falling from a boulder. Or when you fall on your way from or to the crag.
You’ll notice acute pain in your wrist and difficulty moving your hand. In the case of an open fracture, yes, you might see some actual bone sticking out of your wrist.
Since a fracture is an acute injury, the best way to prevent it is by managing the situations where it can happen. This leads me to recommend you the following:
- Practice falling, both on sports routes and on boulder problems. And then all types of boulder problems, slabby, vertical, overhanging, and roofs, and of course from different heights. All of them require you to move your body differently for a safe landing.
- Watch your step on your approach or way back from the crag.
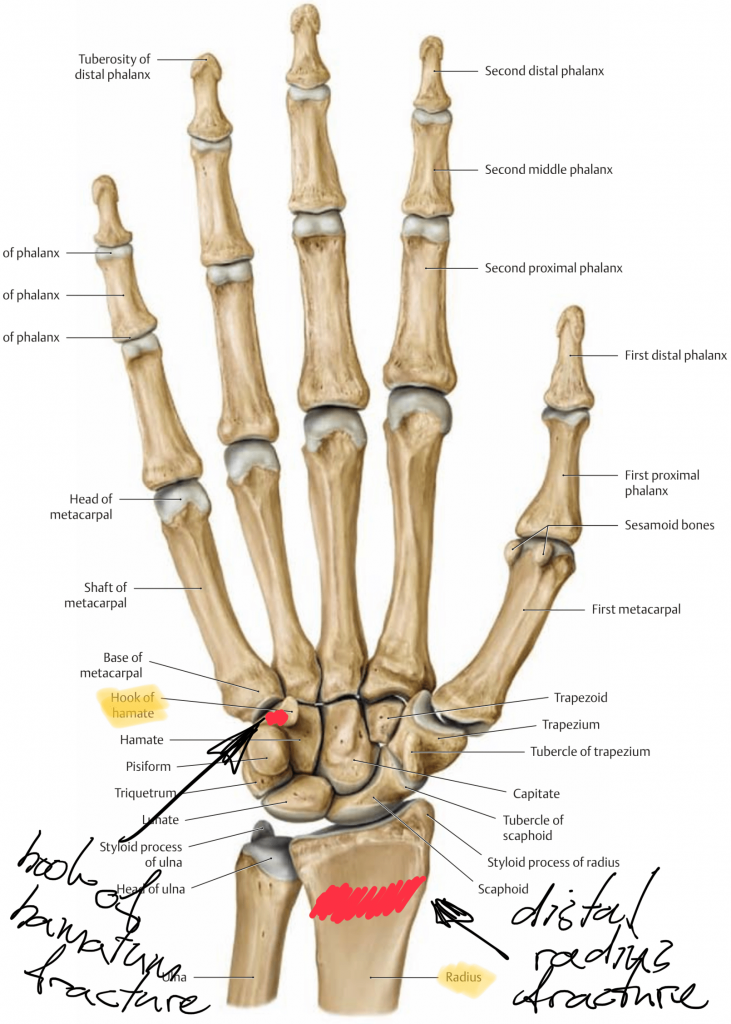
3. Fracture of the Hamate Bone
A fracture of the Hamate bone either happens through hitting something hard with your hand, like falling to the floor, or through a sudden pull like that of your bike steer.
In rock climbers though, a fracture of the hamate bone is more often a consequence of overload. The flexor carpi ulnaris muscle inserts onto the hamatum and is loaded intensely when the hand is in ulnar deviation. Add to that repeated loading of the pinky finger and the ring finger and there’s a risk of Hamate fractures.
Usually, the onset of the pain is slow (so there’s no acute fracture from one day to another!). Also, you can reproduce your pain when you make an ulnar deviation of your hand and then try to bend your pinky finger and ring finger against strong resistance. Do it again but now with your hand deviated radially and your pain should be less.
If you suspect a fracture of the Hamate stop all loading of the hand and do an MRI to confirm the diagnosis. When the MRI confirms the diagnosis you should rest for 6-8 weeks to let it grow back together. Then, follow a loading program for 8-16 weeks to get you back to your original climbing level. Depending on the severity of your injury the time to get back to your original climbing level might be different.
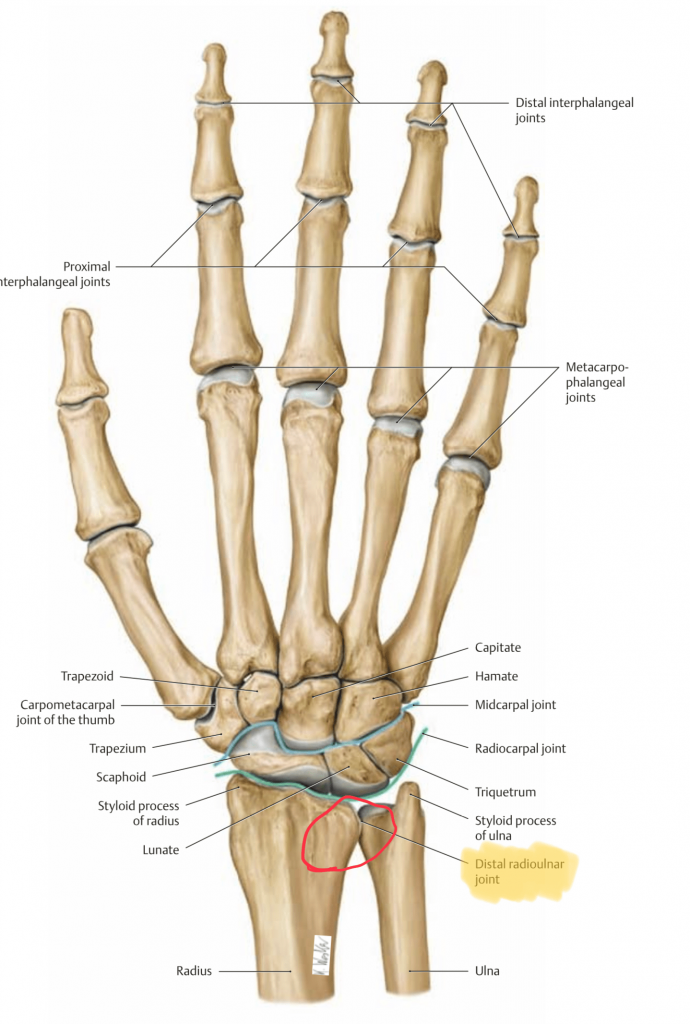
4. Bone Marrow Edema
Bone marrow edema (BME) is a consequence of repetitive strain on the bones in your hand. On the site of the injury, there’s usually an accumulation of water and increased blood circulation.
Repetitive use of your hand and wrist in unnatural positions causes frequent sheer forces on your distal radius, ulna, or carpals. Since the onset of BME is slow, you won’t experience a lot of pain suddenly, but rather an increase in pain over a prolonged period.
See the image below for the region where BME occurs most often.
There are a variety of categories of Bone Marrow Edema:
- Mechanical Bone Marrow Edema can be a result of fractures, overload, misalignments of joints, and degeneration.
- Ischemic Bone Marrow Edema, is the consequence of blood circulation issue which reduces the oxygen supply of the affected bone
- Inflammatory Bone Marrow Edema, caused by infections or rheumatoid arthritis
And there are situations where cancerous tissue or an unknown origin causes BME.
In all cases of BME, you must figure it out as soon as possible to prevent stress fractures or necrosis of your bone tissue. It’s hard to diagnose BME with anything else than an MRI, so make sure to do that instead of other types of imaging.
With all BME you must reduce your climbing load. Possibly, stopping entirely depends on the severity and the climbing you do. After the symptoms have diminished you should start a loading program that exposes you step by step to higher climbing intensity.
5. Carpal Tunnel Syndrome
Carpal Tunnel Syndrome (CTS) is pain due to irritation or inflammation of the median nerve which passes through the carpal tunnel. This is a small space between the carpal bones.
If you have CTS, you might notice a loss of sensitivity in the hand (the part that is innervated by the median nerve), pins and needles in the same area, and a loss of strength in the hand, mostly while grabbing. Furthermore, you might feel pain in the wrist, hand, and sometimes even back up the lower, arm, upper arm, and shoulder. Your pain could be worse at night because you might keep your wrist (unconsciously) bend for long periods.
CTS can be diagnosed clinically based on your history, the type of symptoms, and the use of two tests: the “Tinel Sign” and Phalen Test”. You can read more about CTS in my blog about how to decide between conservative treatment and surgery for carpal tunnel syndrome.
6. Morbus Dupuytren
Morbus Dupuytren is a reaction in the connective tissue in the hand palm. Knobbly tissue is formed, usually in the 4. and 5. line (between your wrist and pinky finger and/or ring finger). This tissue can lead to mobility limitations and pain. Mostly this depends on the position the hand is used in and the stage of the disease.
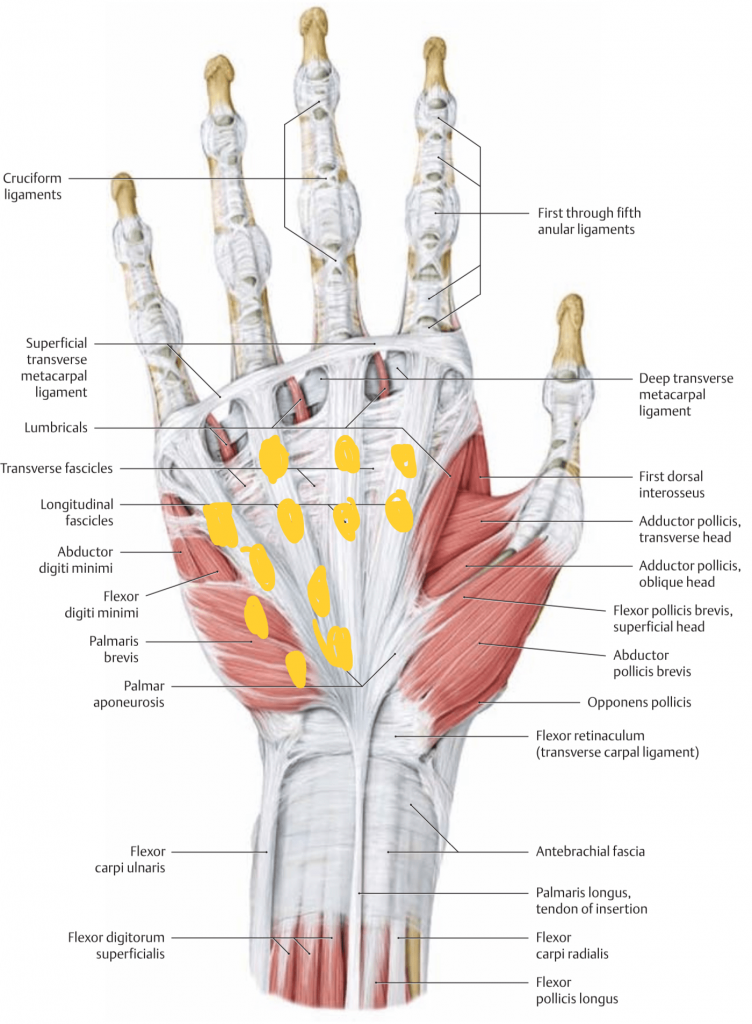
Rock climbing might enhance the onset of Morbus Dupuytren due to repeated microtrauma of the palmar aponeuroses, a sheet of connective tissue that generates tension over the hand palm. Still, the disease often doesn’t progress beyond its initial stage and might therefore not inhibit your rock climbing or your everyday life in a significant way.
If it does limit your climbing, provoke pain, or limit you significantly in your everyday life you can consider surgery to take the extra tissue out.
7. Tenosynovitis
A tendon is a connecting tissue between muscle and bone, and tenosynovitis is a tendon sheath inflammation. This is a tube of connective tissue that helps your tendons slide efficiently. Repetitive overload of a tendon causes increased friction in the sheath which can result in inflammation.
You’ll feel pain along the injured tendon. Since it’s an inflammatory response you’ll likely notice other inflammatory symptoms too: redness, heat, and swelling.
If you have tenosynovitis, you must stop climbing immediately so you won’t aggravate the inflammation. Also, your doctor might prescribe anti-inflammatory drugs. Then, when the worst pain has subsided radial shockwave therapy can help to speed up the recovery process. A splint to stretch the tendon and immobilize the wrist can be helpful to ensure you don’t provoke any pain unwillingly.
When the inflammation is gone you can start a loading program that includes both stretches and exercises that specifically target the injured muscle and tendon. Thus, you must know exactly which tendon is injured so that you can isolate it efficiently with strength exercises. You can increase your training intensity based on the pain during (no more than 4-5/10 and no sharp shooting or radiating pain) and after training (should be gone the next morning).
8. Ulnocarpal Pain Syndrome
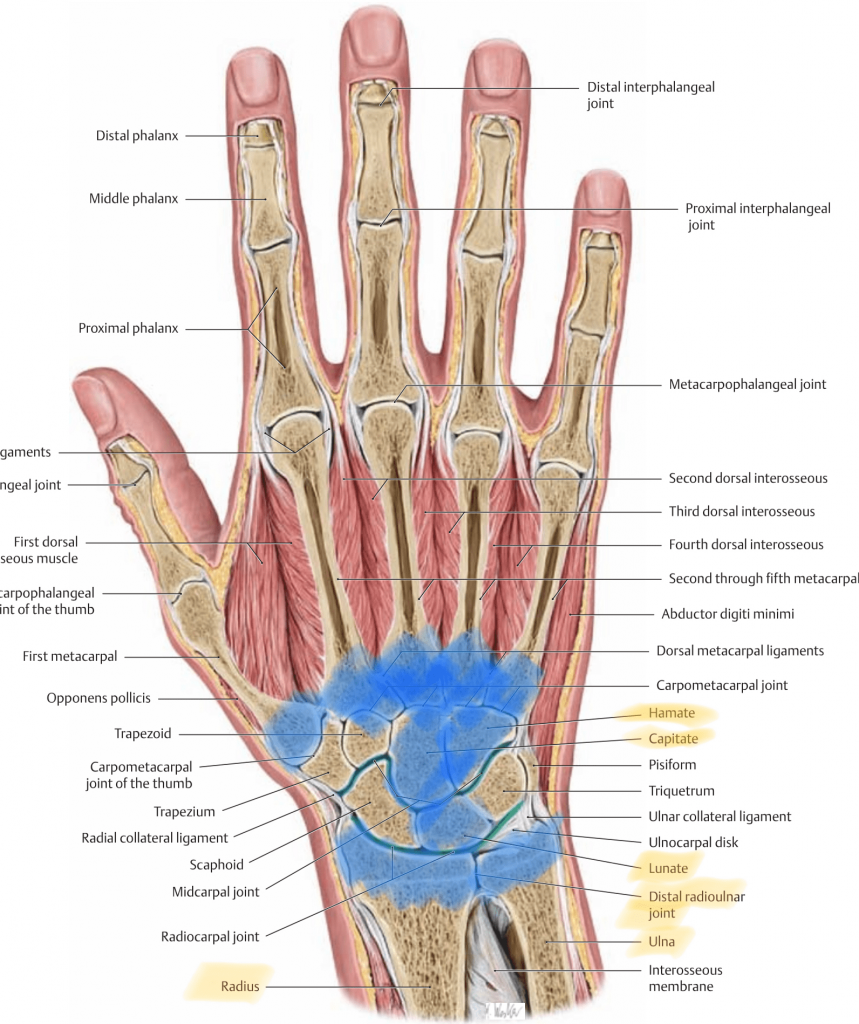
Ulnocarpal Pain Syndrome is a collection of symptoms (that’s why it’s called a syndrome). It can be caused by a variety of structures in the wrist. Ulnocarpal Pain Syndrome implies that the pain is in the ulnocarpal region.

You might feel unstable in your wrist with or without pain. Usually, you feel this pain and instability in the distal radioulnar joint (DRUJ). This is the joint where the radius and ulna meet in front of the carpal bones.
It could be the case however that your pain comes from somewhere in the surrounding structures.
For example:
- Lesions of the triangular fibrocartilage complex
- Synovitis with plica syndrome
- Overload around the Extensor Carpi Ulnaris tendon
- Triquetral impingement ligament tear, or “TILT”-Syndrom
- Carpal instability
- Subluxation of the DRUJ
- Lesions of the lunotriquetral ligament
The bottom line is that an ulnocarpal pain syndrome is a syndrome. This entails that it’s a collection of symptoms that don’t necessarily need a distinct origin to exist. This makes the condition harder to treat. However, if there’s clear synovitis, which is most likely in this situation, an injection with corticosteroids can help. Otherwise, reducing your training load and tracking it with the Rockshoulders Training Log and taping the wrist are good places to start.
After your initial irritation has subsided and you can load your wrist without having irritations or pain responses longer than 6-12 hours, it’s a good idea to train your coordination in the wrist combined with local stability exercises. Also, since ulnocarpal pain syndrome is such an unclear diagnosis, I think it’s important to look at the entire kinetic chain, from your back, neck, and scapula to your fingers. Movement limitations in other joints can force your wrist into painful positions unnecessarily.

